When the Elbow Has Nothing Left to Hold Onto: Rebuilding Stability After Complete Internal Degloving
A case of catastrophic elbow dislocation — and how synthetic ligament reconstruction gave a patient her arm back.
Some injuries look straightforward on the outside — and reveal their true complexity only in the operating theatre.
This is the story of one such case.
The Patient
A 45-year-old woman came to us after sustaining a severe right elbow dislocation. The joint had already been reduced — put back into place — at another hospital. On paper, the X-ray looked acceptable. But the elbow remained dangerously, worryingly unstable. Every time the arm was moved, the joint threatened to dislocate again.
She was referred to our unit at Max Smart Super Speciality Hospital, Saket, for further evaluation and management.
What We Found
Under anaesthesia, we formally tested the elbow — applying careful stress to assess the integrity of the supporting ligaments. The result was alarming. The joint was unstable in every single direction: side to side, front to back, and rotationally. There was no firm endpoint. The elbow had essentially lost all its passive support.
We decided to explore surgically.
What we found inside was something we rarely encounter: the distal humerus — the lower end of the upper arm bone that forms the elbow joint — was completely bare. Every soft tissue structure that normally anchors to this bone had been ripped away by the force of the original injury.
That meant:
• The Medial Collateral Ligament (MCL) — which stabilises the inner side of the elbow against valgus (outward bending) stress — was gone.
• The Lateral Ulnar Collateral Ligament (LUCL) — which stabilises the outer side and prevents the forearm from rotating away from the humerus — was gone.
• The anterior capsule — the tough fibrous envelope at the front of the joint — was also completely stripped.
There was nothing left to repair. No tissue to stitch back. The bone was, quite literally, bare.
“The distal humerus was completely bare — no ligaments, no capsule. There was nothing left to repair. We had to rebuild the joint’s stability from scratch.” — Dr Vikas Gupta
Understanding the Anatomy: Why These Ligaments Matter So Much
The elbow is not a simple hinge joint. It performs two distinct movements — bending (flexion/extension) and forearm rotation (pronation/supination) — and it does so while bearing significant load during everyday activities.
Three soft tissue structures are critical to keeping the elbow stable:
The MCL (medial collateral ligament) runs along the inner side of the elbow and is the primary restraint against the forearm being pushed outward. It is the ligament that pitchers famously tear in baseball — often managed with ‘Tommy John surgery’.
The LUCL (lateral ulnar collateral ligament) runs along the outer side. Its most important role is preventing a specific pattern of instability called posterolateral rotatory instability — where the forearm literally rotates away from the humerus, causing the elbow to subluxate (partially dislocate) with everyday movements like pushing up from a chair.
The anterior capsule provides additional front-to-back constraint. When all three are lost simultaneously, the elbow has virtually no passive stability at all.
The Solution: Synthetic Ligament Reconstruction
Conventional reconstruction in this situation would involve harvesting a tendon graft from elsewhere in the body — the palmaris longus tendon in the forearm, for example, or the gracilis tendon from the thigh — and fashioning new ligaments from it. This is effective, but it comes with donor site morbidity, limited graft availability, and most importantly, a biological maturation period during which the graft must be protected from loading. That typically means several weeks of immobilisation — deeply problematic for an elbow, which stiffens rapidly when kept still.
We chose a different approach.
We used the Xiros Infinity Loop — a synthetic ligament device manufactured by XIROS Ltd (UK), made from high-strength braided polyethylene terephthalate (PET). Its defining feature is a continuous loop architecture: rather than a single strand with two knotted ends, the implant forms an unbroken loop, distributing load evenly along its entire length and eliminating the stress concentration that occurs at fixation knots.

The reconstruction was performed as follows:
LUCL and MCL reconstruction done By drilling the transverse tunnel through the distal humerous and another tunnel through proximal ulna INFINITY loop was passed through both tunnels and tied on itself.
Anterior Capsule Reconstruction: The anterior capsule was also reconstructed using NON absorbable suture through anterior capsule and endobutton fixation on proximal ulna, restoring the front-to-back constraint of the joint.
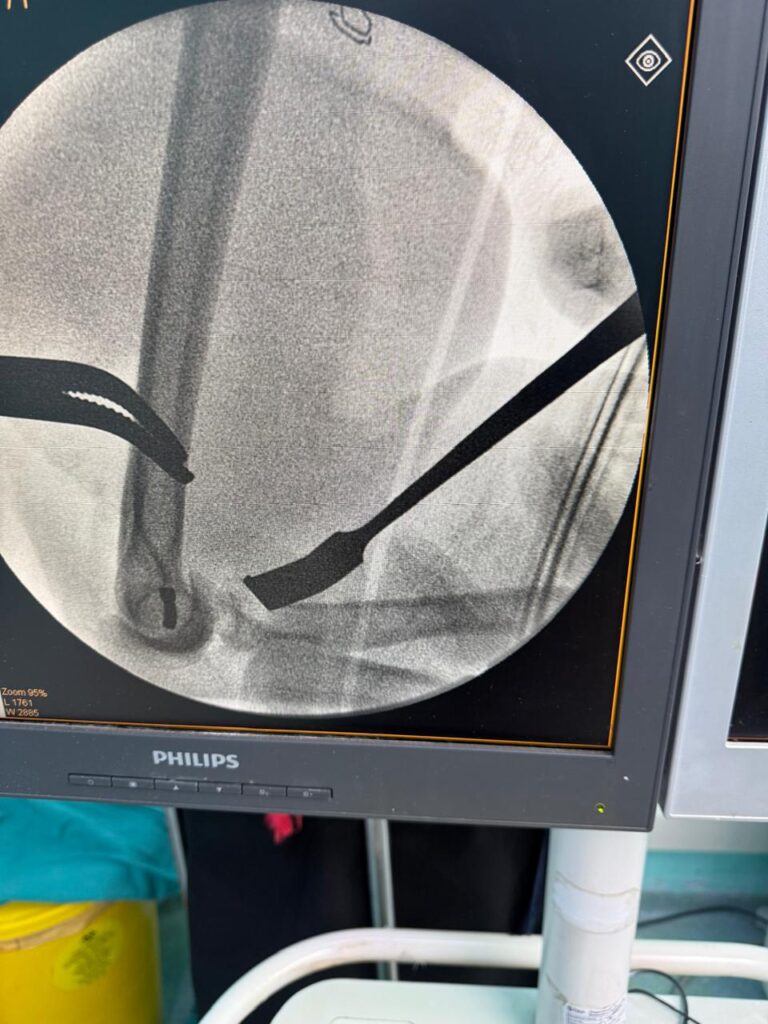
At the end of the procedure, the elbow was tested under fluoroscopy (live X-ray). It was stable — completely stable — in all planes of movement.
The elbow is one of the most stiffness-prone joints in the body. Moving it early — within the first 24 hours — is not just helpful. It is essential.
Moving the Very Next Day
One of the most significant aspects of this case was the rehabilitation timeline.
Unlike a biological graft, a synthetic ligament provides immediate mechanical stability from the moment of fixation. There is no ‘ligamentisation’ period — no phase during which the implant is biologically integrating and must be shielded from load. This means that mobilisation can begin almost immediately.
Our patient began active-assisted range of motion exercises within 24 hours of surgery, under the guidance of our physiotherapy team. She was fitted with a hinged elbow brace to protect the reconstruction while allowing controlled movement.


This early start to rehabilitation is critically important. The elbow joint is notoriously prone to developing stiffness after injury or surgery. Scar tissue forms quickly. Capsular contracture — where the joint capsule tightens and restricts movement — can develop within days of immobilisation. By moving early, we significantly reduce this risk.
At follow-up over the subsequent weeks, the patient demonstrated progressive improvement in range of motion and elbow stability, with no complications.
Why This Case Is Unusual
Complete traumatic internal degloving of the distal humerus — where the bone is stripped entirely bare of soft tissue attachments — is an exceptionally rare finding. Most complex elbow dislocations, even severe ones, leave some residual tissue that can be repaired or augmented.
The use of the Xiros Infinity Loop for acute bilateral elbow collateral ligament reconstruction (MCL + LUCL + capsule) in this setting has, to our knowledge, not been previously described in the published medical literature. We are preparing a formal case report for submission to an international peer-reviewed journal.
What This Means for Patients
If you or someone you know has sustained an elbow dislocation that remains unstable after reduction, early specialist evaluation is essential. Not all elbow dislocations are equal — and the degree of internal soft tissue injury can only be fully assessed with the right expertise and, where necessary, surgical exploration.
Modern synthetic ligament systems have expanded what is surgically achievable in complex upper limb instability. Cases that would once have been managed with prolonged immobilisation — or accepted as permanently unstable — can now be reconstructed with precision, with the goal of early mobility and full functional recovery.
At Hand2Shoulder Clinic and Max Smart Super Speciality Hospital, we treat the full spectrum of elbow conditions — from simple sprains to the most complex reconstructive challenges. If you have an elbow problem that has not been resolved, we are here to help.