When a Bony Growth Near the Shoulder Causes Numbness in the Hand: A Medical Student’s Story
Imagine being 21 years old, at the peak of your academic ambitions, in the middle of your MBBS, and your hand starts going numb. Not from sleeping in an awkward position. Not from too much typing. But from a large, silent tumour quietly growing near your shoulder — pressing on nerves you hadn’t even heard of yet.
That was the reality for one of my patients, a second-year medical student who came to me with a troubling combination of symptoms: progressive numbness in his hand and a vague ache around his upper arm, especially when he raised it overhead. He had been managing it for months, attributing it to long study hours and stress. It was only when his grip began to weaken that he — a medical student, no less — finally decided it was time to see a specialist.
What We Found: A Giant Osteochondroma at the Proximal Humerus


On examination, I could feel a large, hard, non-tender mass arising from the upper end of the arm bone — the proximal humerus. The X-ray confirmed what I suspected.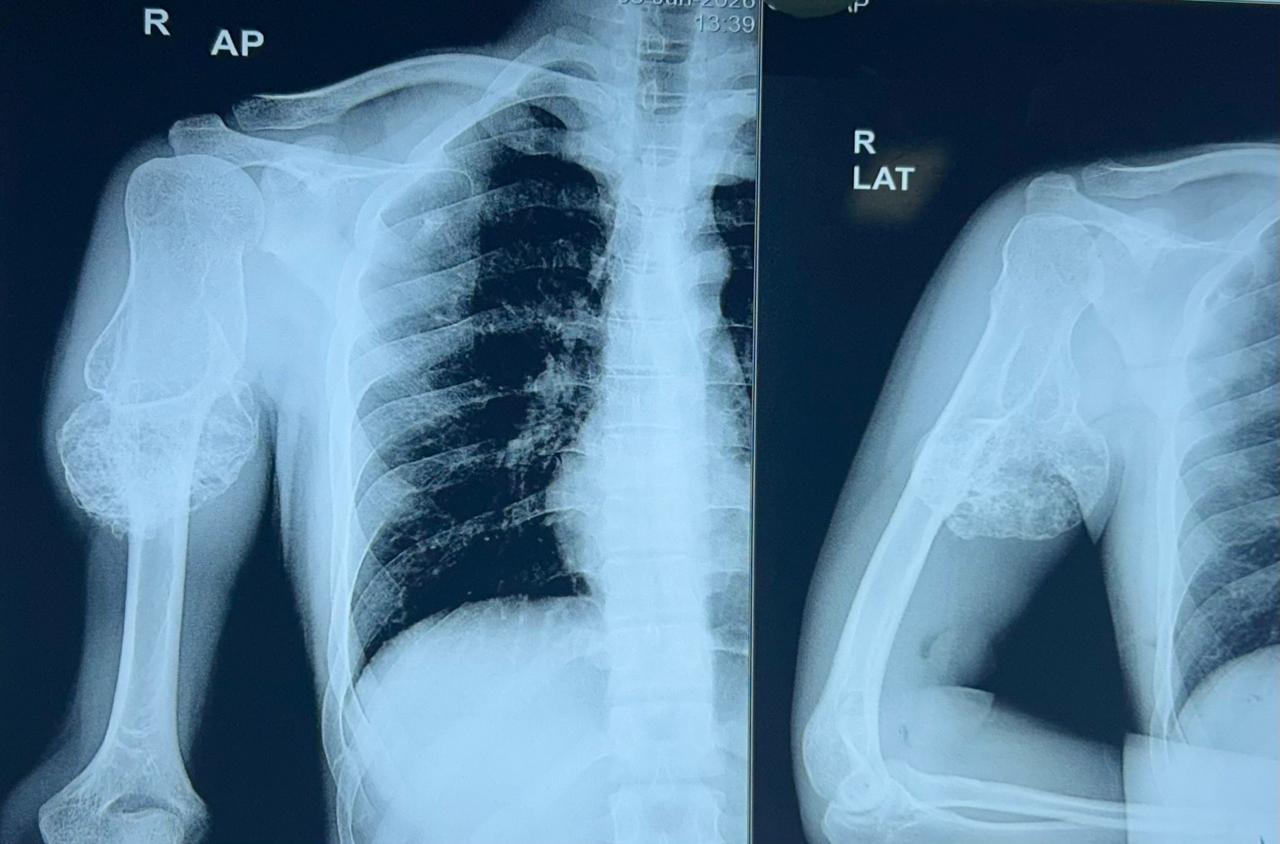
X-ray showing the large osteochondroma arising from the proximal humerus. The bony stalk and cartilage cap are clearly visible, with the tumour projecting medially toward the neurovascular bundle.
The lesion was a classic **osteochondroma** — the most common benign bone tumour — but it was anything but small. It had grown to a substantial size and was projecting in a direction that compressed the **brachial plexus**, the network of nerves that runs from the neck into the arm and controls sensation and movement in the entire upper limb. This explained the numbness and tingling in his fingers perfectly.
What Is an Osteochondroma?
An osteochondroma is a benign outgrowth of bone capped with cartilage. Think of it as a bony bump that grows outward from the surface of a bone, usually near a growth plate. They are most commonly seen in young patients — teenagers and young adults — precisely because they arise from actively growing bone. The proximal humerus (the upper end of the arm bone, just below the shoulder joint) is one of the most frequent sites.
Most osteochondromas are harmless and cause no symptoms. They are often found incidentally on X-rays taken for some other reason. However, when they grow large, or grow in an unfortunate direction — toward blood vessels, nerves, or tendons — they can cause significant problems. In this young man’s case, the tumour had grown medially, directly into the path of the brachial plexus.
The Decision to Operate
In many patients, osteochondromas can simply be watched. But this patient had three clear indications for surgery:
1. Progressive neurological symptoms — numbness and weakness in the hand that were getting worse, not better
2. Significant tumour size — the mass was large enough to be palpable and was compressing vital structures
3. Impact on daily function — the numbness was affecting his ability to write, study, and perform the tasks of a medical student
We counselled him thoroughly. We explained that the surgery involved careful excision of the tumour at its base, which was arising from the proximal humerus, while meticulously protecting the surrounding nerves and blood vessels. He was young, fit, and motivated — an ideal surgical candidate.
Surgery: Complete Excision of the Tumour
Under general anaesthesia, through a carefully planned approach to the proximal humerus, we excised the osteochondroma in its entirety. The tumour, when removed, was truly impressive in size.
The excised osteochondroma specimen. The bony stalk and glistening cartilage cap are visible. The sheer size of this tumour explains why it was compressing the brachial plexus so significantly.


The key principles of surgery were:
– Complete excision at the base — leaving any remnant of the cartilage cap risks recurrence
– Nerve protection — the brachial plexus branches in this region were carefully identified and preserved throughout
– Haemostasis — meticulous control of bleeding from the rich vascular bed around the proximal humerus
The procedure went smoothly. The nerves, though compressed, were intact and undamaged — a reassuring finding that suggested good potential for rapid recovery.
Recovery: Three Days to Relief
Outcomes in nerve compression surgery can sometimes take weeks or months to manifest, as nerves recover slowly. What made this case gratifying was how quickly this young man responded.
Within 72 hours of surgery, he reported that the numbness in his hand had almost completely resolved. The tingling was gone. His grip strength was returning. He could feel the difference from the moment he woke up in the recovery room — the sensation in his fingers was already improving.
This rapid recovery is explained by the nature of the compression. When a nerve is compressed by an external mass (rather than damaged by disease, diabetes, or direct trauma), removing that compression allows the nerve to spring back quickly, provided the compression has not been present long enough to cause permanent structural damage to the nerve fibres. In this patient, the compression was significant but had not crossed that threshold. Early surgery had made the difference.
What This Case Teaches Us
This story carries several important lessons — perhaps especially meaningful coming from a young man who is training to be a doctor himself.
1. A hand problem may originate far from the hand. Numbness and tingling in the fingers are often assumed to be due to carpal tunnel syndrome or cervical disc disease. But the entire pathway from the neck to the fingertips needs to be assessed. A tumour at the shoulder can cause hand symptoms that look no different from a wrist problem.
2. Bony lumps near joints in young people need evaluation. Many patients — and even some doctors — dismiss hard, non-tender swellings in young people as “just bone” or “a harmless growth.” While osteochondromas are usually benign, their location and size determine whether they need treatment.
3. Neurological symptoms should never be ignored or deferred. This patient had lived with worsening hand numbness for months. Had he waited longer, the nerve compression could have progressed to the point where recovery would have been incomplete. The fact that he recovered so quickly after surgery is partly because we operated in time.
4. Surgery for benign bone tumours, in experienced hands, is safe and effective. There is often anxiety — understandably — about operating near the shoulder, where major nerves and blood vessels run close together. Specialised training in upper limb and microsurgery makes all the difference in navigating this anatomy safely.